
- ZocDoc
- RateMD
- Yelp
- Vitals
- Healthgrades
- Birdeye
Meta Description – A detailed guide to apicoectomy surgery for patients and caregivers
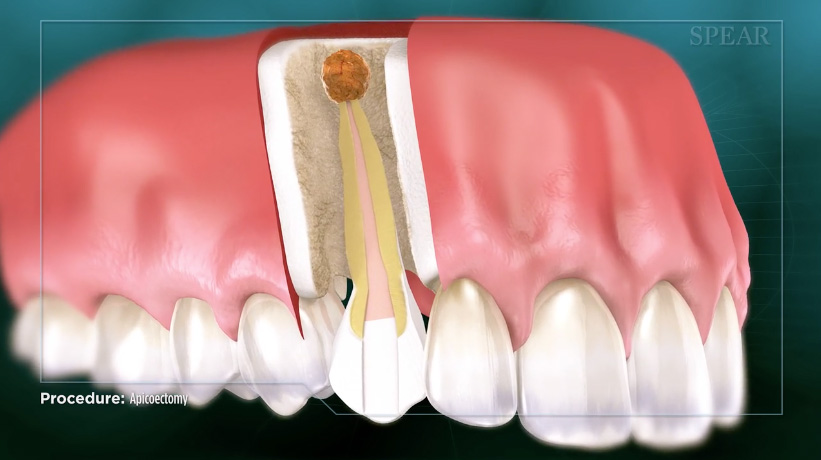
What is an apicoectomy?
Definition of Apicoectomy
An apicoectomy is an endodontic surgery. It is a dental procedure to treat apical periodontitis or inflammation of the roots of a tooth or a tooth abscess. An apicoectomy is prescribed in cases in which root canal therapy has already been performed once (primary root canal therapy), or twice (nonsurgical root canal re-treatment or retreatment therapy) but has not been effective. Rarely, an apicoectomy is prescribed after an initial root canal therapy (1).
Indications for an Apicoectomy
Indications for an apicoectomy include situations with persistent or refractory infection of a root canal system, which could be attributable to a variety of reasons. For instance, a persistent infection might result from iatrogenic changes to the original canal anatomy (2) or the presence of microorganisms in proximity to the terminal end of the root structure where the root meets the ligaments that attach it to the surrounding bone tissue (3 & 4). Other reasons include the existence of an extraradicular infection, which is essentially bacterial plaque on the outside surface of a terminal of the root end surface (5) or bacteria within the lesion, or an abscess that might be present at the junction of the root’s terminal and surrounding structures. (6–9, 17).
The Purpose of Apicoectomy Dental Surgery
The goal of the dentist performing an apicoectomy is to attain complete healing at the junction of the tooth, the apex of the root, and the immediate surrounding bone structure, all of which constitute the “periapical area” (peri = surrounding, the apical = area associated with the apex of the tooth).
The Purpose of Apicoectomy Dental Surgery
The goal of the dentist performing an apicoectomy is to attain complete healing at the junction of the tooth, the apex of the root, and the immediate surrounding bone structure, all of which constitute the “periapical area” (peri = surrounding, the apical = area associated with the apex of the tooth).
Evolution of Apicoectomies as a Treatment
The Traditional approach to apicoectomies has been a prevalent technique for decades. In the Traditional approach, the root ends are exposed surgically and then cut with surgical burs. Mercury-based dental amalgam is then used to fill the root ends in direct contact with bone.

Endodontic Microsurgery is the modern approach to periradicular surgery or surgeries involving only the roots of a tooth. Endodontic Microsurgery is performed under high-power medical microscopes with dedicated illumination devices, utilizing microsurgical instruments, modern ultrasonic preparation of root ends and filling with biocompatible materials such as MTA and bioceramics, to name a few (10).

Considering the fact that many published studies have detailed the benefits of Endodontic Microsurgery as opposed to Traditional techniques, it is surprising that the Traditional techniques are still widely used in the oral surgery and maxillofacial surgery community.
A Dutch survey done in 2008 showed that oral surgeons use amalgam as a root-end filling material 35% of the time and use IRM, a restorative material first introduced in the 1890s, even more often than that (11). At the time the survey was conducted, MTA was recommended as the most biocompatible root-end filling material available, but the study found that oral surgeons only employed MTA at a rate of 2.6%.
Differences in Apicoectomy Techniques
The Traditional approach to apicoectomies differs significantly from Endodontic Microsurgery in the way it goes about trying to achieve the goal of periapical healing. Significant differences include the access armamentarium (standard size surgical burs versus bone cutting burs or piezo tips that minimize surgical trauma) (17); the size of the osteotomy window into the bone (large versus small); the use of micro-instruments that allow better access and visualization of the surgical field; the angle of the root-cutting (acute versus shallow); the root-end preparation (bur versus ultrasonic devices); the direction of preparation (off-angle versus aligned); the root-end repair material (dental amalgam versus better biocompatible material); and most importantly, the tremendously greater ability to identify defects, micro-fractures, additional canals, and root anomalies that led to the root canal failure in the first place under the high-power magnification of a microscope (10).
Outcome Assessment and Success Rates
In order to make an informed decision for clinical care, it is best that one use the highest quality evidence of a positive outcome for a given therapy. In the field of medicine, meta-analyses are of significant value (13).
A meta-analysis of 12 studies (combined sample size, n = 925) that have employed Traditional apicoectomy technique showed a weighted pooled success rate of 59%, while the Endodontic Microsurgery technique performed in 9 studies (n = 699) showed a success rate of 94% (93.52%; 95% CI, 0.8889–0.9816). In essence, the probability of success for Endodontic Microsurgery technique was 1.58 times the probability of success for the Traditional procedure. The odds ratio indicated that Endodontic Microsurgery had 10.01 times the odds of success.
Endodontic Microsurgery’s cumulative success rate of 93.52% (17) lies exactly in the range of initial endodontic treatment, which has a success rate of 93.5% (14) and restored single unit implants, which has a success rate of 95% after six months (15). The odds of success of an alternative treatment option—non-surgical root canal retreatment—is also similar to the above numbers.
It is essential to avoid making clinical decisions as to which course of therapy to take purely based on mathematical numbers. One should never use these success rates as a justification to use the surgical approach immediately instead of non-surgical approaches (retreatment of root canal therapy) when the option is available. While mathematical numbers might look the same, the clinical picture and the degree of benefit to the patient’s quality of life might differ greatly.
Factors That Influence a Successful Outcome
Under certain clinical circumstances, either the nonsurgical treatment approach or the surgical approach might be the sole indicated treatment (1). Some considerations include whether the original root canal anatomy can be reentered, whether the root canal system is accessible, and the particular dental history of the teeth involved.
Last, it has to be stressed that for endodontic surgery, a successful outcome in terms of healing of the existing periapical pathology, together with a good long-term prognosis of the tooth, depends on good case selection by the endodontist. Limiting Endodontic Microsurgery primarily to teeth where the disease can conclusively be attributed solely to endodontics improved the outcome significantly. When other disease processes were the primary etiology, such as periodontal diseases, tooth decay, or restorative shortcomings, the authors of more robust studies avoided recommending Endodontic Microsurgery as a treatment option. This highlights the significance of having a correct diagnosis and the true etiology of the disease process before committing to a procedure.
Choice of Practitioner in Apicoectomy and Alternative Options
Increasingly, advanced specialization makes it difficult for one practitioner to keep abreast of developing techniques in other specialties. It has been shown that practitioners of different specialties go about treating the same problem differently. This has been demonstrated even for initial root canal therapy (16) as well as for re-treatment of initial root canal therapy (retreatment therapy) (unpublished data, Setzer et al 17).
Setzer claims that, in situations where a root canal or retreatment is indicated to save the natural tooth, specialists who are primary implant providers recommended tooth extraction and placement of a dental implant instead of endodontic therapy whereas endodontists advocated preserving the natural tooth. Among general practitioners, there was a more even distribution among cases in which they recommended endodontic therapy versus extraction and implant. (17).
Apicoectomy: Cost Analysis
All else being equal, the cost of an apicoectomy dental surgery by a specialist or a dentist is generally lower than the cost of an extraction followed by the placement of a dental implant and a prosthetic crown restoration. Assuming proper case selection, an apicoectomy is performed on a tooth that already has an intact and functioning prosthetic crown, thereby negating the need for the further expense of restoration. Furthermore, an extraction might also need to be followed by ridge preservation techniques before a dental implant may be placed and the cost of the dental implant fixture itself must be taken into account.
Apicoectomy Versus Dental Implants
In terms of the time cost involved, apicoectomy dental surgery is a one-visit procedure, while the combination of extraction therapy, ridge preservation procedure and dental implant placement spans four to eight months and involves several shorter procedures. While dental implants are an excellent treatment option within dentistry, they should really be considered a treatment of last resort when a tooth cannot be saved any other way.
Endnotes:
Significant parts of this document are based upon the superb paper by Setzer FC, et al (17)
- ZocDoc
- RateMD
- Yelp
- Vitals
- Healthgrades
- Birdeye
- ZocDoc
- RateMD
- Yelp
- Vitals
- Healthgrades
- Birdeye










