
- ZocDoc
- RateMD
- Yelp
- Vitals
- Healthgrades
- Birdeye
Meta Description – A detailed guide to apicoectomy surgery for patients and caregivers
At a Glance
-
Apicoectomy is a dental surgical procedure to remove the tip of the tooth root
Patients usually have apicoectomy if they fail to find relief after root canal or have persistent root inflammation
Apicoectomy success rate is 94% in properly selected patients who undergo endodontic microsurgery
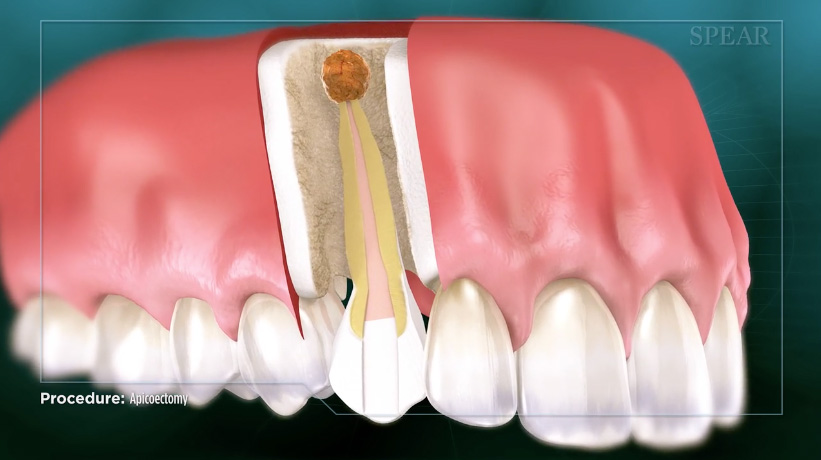
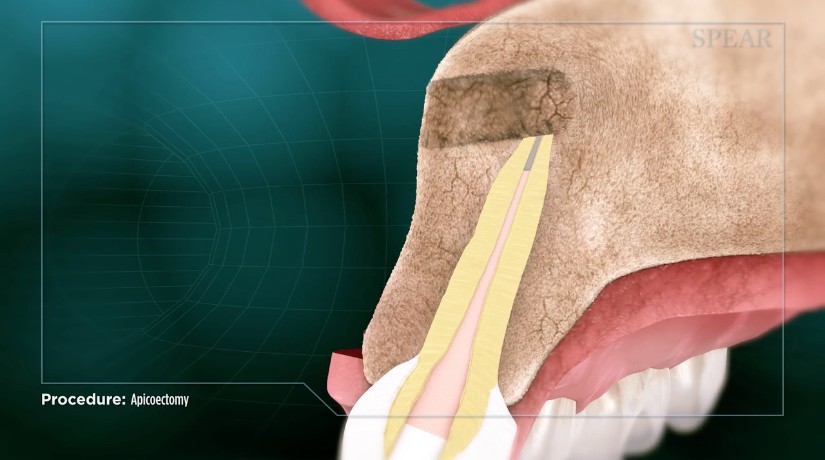
What is an apicoectomy?
An apicoectomy is a dental surgical procedure to remove inflamed tissue at the tip of a tooth’s root. During an apicoectomy procedure, the endodontist makes a small incision at the gums and retracts the tissue to visualize the affected area. A small amount of bone and all diseased tissue are then removed. Any remaining root tissue is also removed during apicoectomy, and a small filling is placed at the root end. Indeed, apicoectomy is commonly known as root-end surgery because the focus of the intervention is the junction between root and bone.
Is apicoectomy right for me?
Indications
An apicoectomy is usually reserved for patients who continue to have apical periodontitis after nonsurgical treatment (Karabucak & Setzer, 2007). In other words, the gums at the root end are continually inflamed despite conservative treatments. People who have failed to find relief after a root canal are also candidates for apicoectomy (Karabucak & Setzer, 2007).
Alternatives
Since apicoectomy is usually reserved for patients who have not found relief from other, nonsurgical treatments (Kui, Labunet, Popescu, Popa, & Lascu, 2018), there are few true alternatives. The main alternative to apicoectomy is to simply extract the tooth itself. The tooth extraction removes the root and also allows the dentist to remove infected or inflamed tissue beneath. The extracted tooth is then replaced with a dental implant, bridge, or denture.
Weighing the Pros and Cons of Apicoectomy and Extraction

The major advantage of apicoectomy over extraction is that patients are able to preserve their natural tooth, which is far preferable to implants or dental appliances (von Arx, 2011). Tooth loss causes esthetic, psychological and social problems for many patients (Davis, Fiske, Scott, & Radford, 2000; Okoje, Dosumu, Alonge, & Onyeaso, 2012), and the natural tooth usually outperforms the implant (Chandki & Kala, 2012). Indeed, a dental implant should only be considered as an alternative to a natural tooth when the tooth cannot be saved or when prognosis with a natural tooth is poor (Iqbal & Kim, 2008). Conversely, some professionals argue that tooth extraction with implant is preferable to apicoectomy because it may preserve more of the underlying bone (Ruskin, Morton, Karayazgan, & Amir, 2005). Your endodontist can help you decide the right treatment plan for your specific needs.
Apicoectomy risks
The major risk of apicoectomy is that it simply does not relieve a patient’s symptoms. If the area does not heal or continues to cause pain, this is consistent with apicoectomy failure and is considered a poor outcome. If this occurs, the patient may need a second apicoectomy or the tooth may need to be extracted. If too much bone is removed during apicoectomy, it may prevent the placement of a dental implant in the future. As with any dental surgery, there is a small risk of infection, bleeding, or nerve damage.
What can I expect during and after apicoectomy?
During the procedure
In most cases, the endodontist will use local anesthesia or a nerve block to temporarily deaden sensation in the affected area. Patients who are particularly averse to dental procedures may also receive conscious sedation immediately prior to the apicoectomy procedure. Aside from the local anesthesia injection, you may feel some pressure and vibrations during the surgery. If you experience sharp or intense pain at any point during the apicoectomy (this is exceedingly rare), notify the endodontist immediately as additional local anesthesia may be needed.
After the procedure
As the nerve block wears off, you may experience some soreness and discomfort in the treated area. Your endodontist will give you pain medication to help relieve this discomfort. Minor blood spotting around the apicoectomy treatment area is normal, but heavy bleeding is not. Most people can drive themselves home soon after the apicoectomy procedure. If the patient does need conscious sedation, then he or she will need to arrange transportation home after the surgery. Apicoectomy recovery is usually quite rapid; patients can return to work and regular daily activities the day after surgery.
Outcomes and Prognosis
When performed by an experienced endodontist on properly selected patients, the apicoectomy success rate is quite high. When researchers collected and analyzed results from 21 clinical trials including over 1,600 patients, they found that 59% of patients treated with traditional root end surgery had a positive outcome six months after the apicoectomy procedure (Setzer, Shah, Kohli, Karabucak, & Kim, 2010). On the other hand, 94% of patients who underwent endodontic microsurgery (EMS) for their apicoectomies had a positive outcome. A positive outcome, in this case, was evidence of healing and the absence of pain, swelling, and sensitivity in the affected tooth. Indeed, patients will know they have had a successful apicoectomy if the procedure relieved their pain and related symptoms.
Importantly, only patients who meet certain clinical criteria can expect to enjoy this high apicoectomy success rate. Specifically, disease should be mostly limited to the root/pulp itself. Patients with substantial gum and bony disease are probably not good candidates for apicoectomy (Kim, Song, Jung, Lee, & Kim, 2008). Because apicoectomy success rates are substantially higher with endodontic microsurgery than traditional root end surgery, most professionals and patients opt for the microsurgical approach.
Who performs an apicoectomy?
An apicoectomy is performed by endodontist, which is a surgeon who specializes in surgery of the dental pulp including the tooth root. These dental specialists complete two years of additional training beyond general dentistry specifically to treat diseases of the pulp and root. Since most modern apicoectomies involve endodontic microsurgery, patients should select an endodontist capable of performing microsurgery, i.e., surgery under a microscope.
- ZocDoc
- RateMD
- Yelp
- Vitals
- Healthgrades
- Birdeye
- ZocDoc
- RateMD
- Yelp
- Vitals
- Healthgrades
- Birdeye










